Odovtos-International Journal of Dental Sciences (Odovtos-Int. J. Dent. Sc.), Online First, 2025. ISSN: 2215-3411
https://doi.org/10.15517/njyzcs24

https://revistas.ucr.ac.cr/index.php/Odontos
CASE REPORT:
Dental Findings in Goltz Syndrome: A Case Report and Literature Review
Hallazgos dentales en el síndrome de Goltz: reporte de un caso y revisión de la literatura
Adriana De la Torre¹ https://orcid.org/0009-0007-1421-7453
Santiago Torres-Morales² https://orcid.org/0009-0003-1757-2152
Juan Pablo López Salazar3 https://orcid.org/0000-0003-0671-1543
Alexandra Mariño² https://orcid.org/0009-0002-1749-1304
Laura Sanabria² https://orcid.org/0009-0006-2653-7254
¹Odontóloga pediatra. Departamento de Crecimiento y Desarrollo, Hospital Universitario Fundación Santa Fe de Bogotá, Colombia.
²Facultad de Odontología, Universidad El Bosque, Colombia.
3Cirujano Oral y Maxilofacial. Departamento de Salud Oral, Hospital Universitario Fundación Santa Fe de Bogotá, Colombia.
Correspondence to: Santiago Torres-Morales - storresm@unbosque.edu.co
Received: 16-VII-2025 Accepted: 5-IX-2025
ABSTRACT: Goltz syndrome or Focal dermal hypoplasia, is a genetic polymorphic cutaneous disorder with highly variable anomalies affecting the eyes, central nervous system, urinary system, gastrointestinal system, cardiovascular system, and craniofacial and dental complex. It is transmitted as an X-linked dominant trait. Clinical signs include cutaneous atrophy and periorificial papillomas that commonly appear around the mouth, genitals, and/or anus, include onychodystrophy and cicatricial alopecia, bone disorders, such as syndactyly, ectrodactyly, and/or aplasia of fingers in the hands or feet, are present from birth, scoliosis, hypoplastic clavicles and ribs, and thoracic deformation. This syndrome is associated with dental abnormalities that may include malocclusion, oral papillomas, and enamel defects. It affects tissues derived from both the ectomesenchyme. The objective of this study was to provide a narrative review of the oral cavity findings described in Goltz syndrome and present a case report.
KEYWORDS: Goltz syndrome; Focal dermal hypoplasia; Oral manifestations.
RESUMEN: El síndrome de Goltz, o hipoplasia dérmica focal, es un trastorno cutáneo genético polimórfico con anomalías altamente variables que afectan a los ojos, el sistema nervioso central, el sistema urinario, el sistema gastrointestinal, el sistema cardiovascular, así como al complejo craneofacial y dental. Se transmite como un rasgo dominante ligado al cromosoma X. Los signos clínicos incluyen atrofia cutánea y papilomas periorificiales que suelen aparecer alrededor de la boca, los genitales y/o el ano; también se observan onicodistrofia y alopecia cicatricial. Desde el nacimiento pueden estar presentes alteraciones óseas como sindactilia, ectrodactilia y/o aplasia de dedos en manos o pies, escoliosis, clavículas y costillas hipoplásicas, y deformidades torácicas. Este síndrome se asocia con anomalías dentales que pueden incluir maloclusión, papilomas orales y defectos del esmalte. Afecta a tejidos derivados del ectomesénquima. El objetivo de este estudio fue realizar una revisión narrativa de las manifestaciones orales descritas en el síndrome de Goltz y presentar un reporte de caso.
PALABRAS CLAVE: Síndrome de Goltz; Hipoplasia dérmica focal; Manifestaciones orales.
Introduction
Goltz syndrome, also known as focal dermal hypoplasia, is a rare multisystem disorder that follows an X-linked inheritance pattern and is associated with mutations in the PORCN gene, which encodes the enzyme porcupine O-acyltransferase (1). This gene plays a crucial role in embryogenesis, as it is involved in the Wnt/β-catenin signaling pathway, leading to aberrant protein coding in essential tissues such as epithelial and connective tissues (2).
The clinical presentation is characterized by abnormalities in ectodermal, mesodermal, and their derivative tissues. Oral manifestations include malocclusions, ectopic eruptions or impacted teeth, developmental anomalies such as hypoplasia and hypodontia, as well as other abnormalities in tooth size, eruption, and positioning (3,4).
Craniofacial features include facial asymmetry, microcephaly, cleft lip and palate, protrusion and asymmetry of the ears, maxillary hypoplasia, and prognathism (2,3,4,5).
Musculoskeletal involvement includes split hand/foot malformations, deformities in the clavicle, ribs, and long bones, such as the radius, along with syndactyly and scoliosis. Cutaneous abnormalities include nail dysplasia, pigmentation changes, telangiectasias, hypoplastic skin, and alopecia. In addition, neurological alterations have been reported, including developmental delay, microcephaly, and cerebral atrophy (4,5).
These patients require a multidisciplinary approach, involving a medical and dental team from the time of diagnosis as well as throughout treatment and follow-up (4,5). This article presents a case report of a 4-year-old patient, analyzing their clinical and oral manifestations.
Case Report
A 4-year-old female patient, the product of a first pregnancy, born to a 23-year-old mother and a 30-year-old father with no consanguinity, is presented. Delivery was performed via cesarean section at 33 weeks due to a premature placental abruption, which caused placental insufficiency and, ultimately, intrauterine growth restriction or low birth weight for gestational age. The mother reported working on a construction site and being exposed to materials such as cement before pregnancy. She discontinued work during the first trimester.
The patient has been attending the pediatric dentistry department at Fundación Santa Fe de Bogotá, Colombia, accompanied by her mother, since September 2020. She was diagnosed with Goltz syndrome at 5 months of age and presents with complete sequencing of the PORCN gene, showing a c.1093 C>T variant, with no family members having undergone genetic testing. Her medical history also includes intestinal volvulus in 2019, managed surgically without bowel resection, pneumonia in 2022, delayed speech development, astigmatism, nasolacrimal duct obstruction, and hyperpigmented atrophic plaques. The patient is currently undergoing treatment with speech therapy, pediatrics, dermatology, and optometry. During the interview, the mother mentioned that the patient has difficulty chewing and swallowing food, in addition to sensitivity and destruction of the anterior teeth. She has not experienced inflammation or abscesses and had not received dental treatment before 2020.
On extraoral examination, the patient presented with a brachycephalic skull and a convex facial profile (Figure 1). Intraorally, the mucosa appeared pink and shiny. The maxilla was compressed, the tonsils hypertrophic, with a high-arched palate, normal floor of the mouth, and a typically inserted upper labial frenulum. Enamel hypoplasia and defects were observed in the posterior teeth, as well as ectopic tooth morphology. The patient had stainless steel crowns due to previous caries and anterior tooth loss due to decay, resulting in an unstable occlusion and a mesial step molar relationship on the left side (Figure 2 and Figure 3). The panoramic radiograph showed that the patient was in the primary dentition stage, with the ongoing formation of permanent tooth germs (Figure 4). Physical examination revealed ectrodactyly, multiple hypopigmented atrophic plaques on the left lateral trunk following the lines of Blaschko, syndactyly, anonychia, nail dystrophy, and papules in the perioral region (Figure 5). Comprehensive pediatric dental treatment was carried out, including protective stabilization with prior authorization from the mother, due to the patient’s definitively negative behavior, extensive treatment needs, and young age. The treatment included biofilm management, pulpal therapies on primary teeth, basic and advanced restorative procedures, multiple extractions, and maxillary management using a modified Hawley appliance with an esthetic anterior segment (Figure 6). At the end of the treatment, self-care instructions were provided, understood, and accepted by the caregiver. The patient remains under ongoing follow-up.

Figure 1. Profile image. Patient with a convex profile.

Figure 2. Occlusal image.

Figure 3. A. Lower arch. Presence of hypoplasias and enamel developmental defects can be observed. B. Upper arch. The presence of pediatric dentistry treatments can be observed.

Figure 4. Panoramic radiograph of the patient, showing absence of upper deciduous teeth and the right upper second molar.
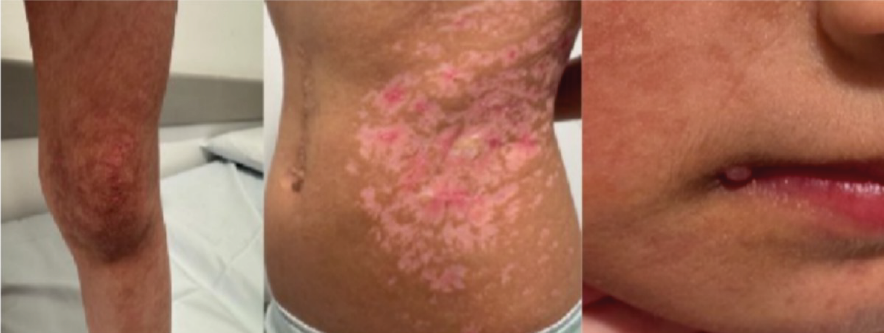

Figure 5. Body images.

Figure 6. Dentofacial orthopedics with modified Hawley appliance with an esthetic anterior segment.
Discussion
Goltz syndrome is caused by a mutation in the PORCN gene located on the X chromosome. To date, approximately 300 or more cases have been reported worldwide, with the majority occurring in females due to the X-linked dominant inheritance pattern, which explains why around 90% of cases are seen in females. However, cases have also been reported in males, although homozygous mutations are typically lethal (6).
The manifestations of Goltz syndrome vary among affected individuals, and many present with only a subset of the characteristic clinical criteria. These include atrophy and hypoplasia of the skin along the lines of Blaschko, hypopigmented or hyperpigmented skin areas, nodular fat herniation, hypoplastic or dysplastic nails, telangiectasias, and papillomatous lesions on mucous membranes such as the mouth, nose, larynx, esophagus, vagina, and rectum. Histopathological findings in skin samples, as reported in the study by Herlin, L. K. et al. (2024), show a hypoplastic and atrophic dermis with disorganized collagen and fat tissue. In contrast, papillomas exhibit hyperkeratosis, papillomatosis, and epidermal hyperplasia. These findings correlate with the clinical lesions. Limb malformations include syndactyly, ectrodactyly, oligodactyly, and congenital absence of hands, arms, forearms, or elbows without distal portions, hemimelia, and shortening of long bones. Dental anomalies are also present, with enamel defects observed in 80% of cases (7,8).
The prognosis and treatment depend on the organs involved. While many cases show normal development, 15% of reported cases exhibit cognitive impairment, but only in those with more severe clinical presentations (9). It is essential not to confuse Gorlin-Goltz syndrome (also known as basal cell nevus syndrome) with Goltz syndrome, as these genetic disorders are often mistaken for one another. Gorlin-Goltz syndrome is caused by mutations in the PTCH1 gene and is characterized by multiple basal cell carcinomas, odontogenic keratocysts, and skeletal anomalies (10).
Oral manifestations occur in more than half of affected individuals. These may include enamel hypoplasia, which predisposes to dental caries. Other reported dental abnormalities include hypodontia, oligodontia, supernumerary and crowded teeth, microdontia, taurodontism, and abnormal tooth and root morphology. Problems with eruption and positioning of teeth in the jaws may also be present (11).
In Colombia, three clinical cases of Goltz syndrome have been documented, none of which report dental management of the affected patients (12). The oral and facial findings described in the literature, as well as those observed in the presented case, include hypodontia, atypical facial morphology, and malocclusions. Therefore, pediatric dental management was essential to recognize these skeletal, muscular, and cutaneous features. The elimination of infectious foci was necessary due to the presence of carious lesions, and regular follow-up was required to monitor the patient’s growth and development. This also allowed for the ongoing identification of oral and maxillofacial findings, as well as the education of the patient’s caregivers on the importance of oral healthcare.
Conclusion
Goltz syndrome is a rare genetic disorder characterized by abnormalities across multiple systems and tissues, including the craniofacial region. There is little or limited scientific evidence regarding its dental management; therefore, guidelines or multidisciplinary teams should be established, including dentistry and its various specialties, to focus on these patients for early diagnosis and management, to prevent disease or control associated risk factors.
Author contribution statement: Conceptualization and design: A.D.L.T. and S.T.M.; Literature review: S.T.M.; Methodology and validation: J.P.L.S.; Formal analysis: J.P.L.S. and S.T.M.; Research and data collection: A.M. and L.S.; Resources: A.D.L.T.; Data analysis and interpretation: A.D.L.T. and S.T.M.; Writing-original draft preparation: A.D.L.T. and S.T.M.; Writing-review and editing: S.T.M.; Supervision: S.T.M.
References
1. Harmsen M.B., Azzarello-Burri S., García González M.M., Gillessen-Kaesbach G., Meinecke P., Müller D., et al. Goltz-Gorlin (focal dermal hypoplasia) and the microphthalmia with linear skin defects (MLS) syndrome: no evidence of genetic overlap. Eur J Hum Genet. 2009; 17 (10): 1207-15. doi:10.1038/ejhg.2009.40
2. Arlt, A., Kohlschmidt, N., Hentschel, A., Bartels, E., Groß, C., Töpf, A., Edem, P., Szabo, N., Sickmann, A., Meyer, N., Schara-Schmidt, U., Lau, J., Lochmüller, H., Horvath, R., Oktay, Y., Roos, A., & Hiz, S. (2022). Novel insights into PORCN mutations, associated phenotypes and pathophysiological aspects. Orphanet journal of rare diseases, 17 (1), 29. https://doi.org/10.1186/s13023-021-02068-w
3. Wang L., Jin X., Zhao X., Liu D., Hu T., Li W., et al. Focal dermal hypoplasia: updates. Oral Dis. 2013; 20 (1): 17-24. doi:10.1111/odi.12083
4. Wright J.T., Puranik C.P., Farrington F. Oral phenotype and variation in focal dermal hypoplasia. Am J Med Genet C Semin Med Genet. 2016; 172 (1): 52-8. doi:10.1002/ajmg.c.31478
5. Nobre Á.V.V., Taba M. Jr., Silva A.R., de Souza S.L.S., Motta A.C.F. Focal dermal hypoplasia (Goltz syndrome): A case report showing a wide variety of systemic and oral manifestations. Ann Dermatol. 2022; 34 (4): 291. doi:10.5021/ad.20.120
6. Gupta, I., Dhankar, N., Dayal, S., & Tyagi, M. (2022). Focal Dermal Hypoplasia (Goltz Syndrome): A Rare Case. Indian dermatology online journal, 13 (4), 502-504. https://doi.org/10.4103/idoj.idoj_663_21
7. Herlin, L. K., Herlin, M. K., Vinter, H., Blechingberg, J., Andersen, B. N., Kruse, C., & Sommerlund, M. (2024). Phenotypes, Genetics, and Estimated Prevalence of Focal Dermal Hypoplasia (Goltz Syndrome): A Single-Center Report. Pediatric Dermatology, 41 (6), 1106-1113. https://doi.org/10.1111/pde.15752
8. Al Kaissi, A., Ryabykh, S., Kenis, V., Ben Chehida, F., Al Kaissi, H., Kircher, S. G., & Grill, F. (2023). Cutaneous, Cranial, and Skeletal Defects in Children and Adults with Focal Dermal Hypoplasia. Children, 10 (10), 1715.https://doi.org/10.3390/children10101715
9. Corona-Guerra G.X., Ochoa-Apreza M. Hipoplasia dérmica focal (síndrome de Goltz). Bol Med Hosp Infant Mex [Internet]. 2018 Jun [citado 2022 Dic 27]; 75 (3): 178-82. Disponible en: http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1665- 11462018000300178. doi:10.24875/bmhim.m18000025
10. Figueira, J. A., Batista, F. R. S., Rosso, K., Veltrini, V. C., & Pavan, A. J. (2018). Delayed Diagnosis of Gorlin-Goltz Syndrome: The Importance of the Multidisciplinary Approach. The Journal of craniofacial surgery, 29 (6), e530-e531. https://doi.org/10.1097/SCS.0000000000004438
11. Nathwani, S., Martin, K., & Bunyan, R. (2018). Focal dermal hypoplasia: A novel finding in disguise. Journal of oral biology and craniofacial research, 8 (2), 143-146. https://doi.org/10.1016/j.jobcr.2018.01.001
12. Acosta J.C., Motta A., Prieto J.C. Hipoplasia dérmica focal (Síndrome de Goltz): amplia variabilidad fenotípica [Internet]. 2009 [citado 2022 Dic 27]. Disponible en: http://hdl.handle.net/10554/45978
 Odovtos -Int J Dent Sc endoses to CC-BY-NC-SA 4.0.
Odovtos -Int J Dent Sc endoses to CC-BY-NC-SA 4.0.